The final frontier of the malaria fight is as much about economics and topography as it is about biology. As temperatures rise, malaria is climbing into highland areas where populations lack natural immunity . Research shows that “U-shaped” valleys in these regions are five times more likely to host parasites than steeper “V-shaped” valleys, as their flat floors provide stagnant water for vector breeding.
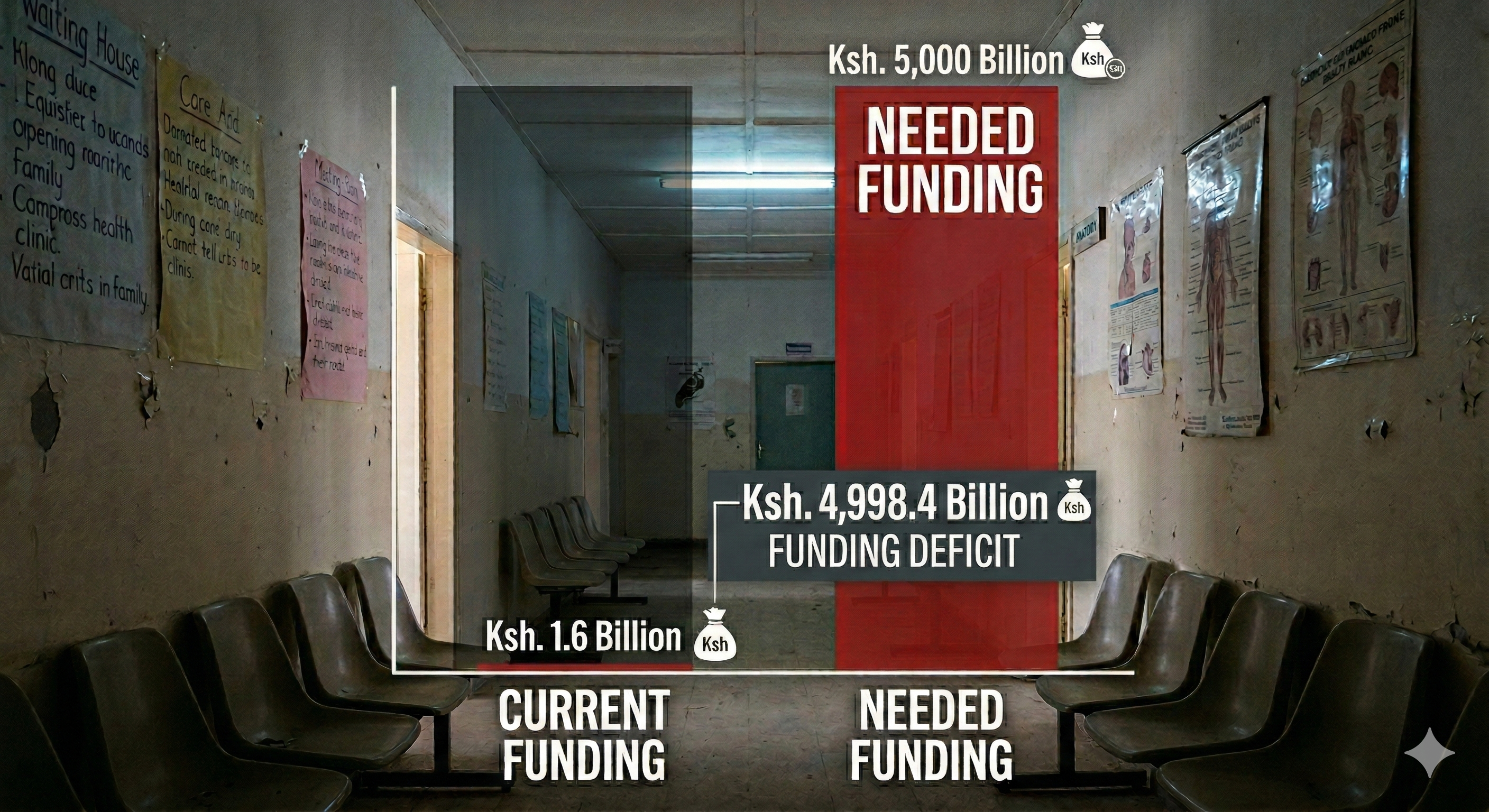
While Kenya’s 2023-2027 strategy aims for a 90% reduction in deaths, these goals are currently balanced on the edge of a financial abyss . In 2024, global malaria funding reached only $3.9 billion—less than half of what is needed annually. Abrupt 2025 US funding cuts have triggered a “cascading collapse” in health infrastructure, with nearly 25,000 community health workers in Kenya facing imminent layoffs .
Without sustainable, government-led financing models, the health system remains vulnerable to unplanned disruptions. To secure a malaria-free future, Kenya must pivot toward local manufacturing of diagnostics and vaccines while integrating climate data into every level of health governance. The line between a breathtaking view of elimination and a dangerous resurgence is currently dependent on filling these “ghost deficits” in aid.
References:
Human Rights Watch Donor Nation Cuts to Global Health Financing Affect Millions
Physicians for Human Rights “The System is Folding in on Itself”: The Impact of U.S. Global Health Funding Cuts in Kenya
Kenya’s role as a pioneer in the Malaria Vaccine Implementation Programme has already saved lives, with a 13% reduction in child mortality observed in pilot regions. We are now entering a new phase with the rollout of the R21/Matrix-M vaccine, which is more cost-effective at approximately $3 per dose and boasts nearly 75% efficacy . Beyond vaccines, the 2025 approval of “Coartem Baby” marks the first treatment specifically formulated for infants weighing as little as 2kg .
However, the effectiveness of these high-tech “shields” is threatened by systemic disconnects. A fourth dose is required in the second year of life to maintain protection, yet many families face logistical and financial barriers to returning to the clinic . There is a persistent risk that advanced tools are being deployed in facilities plagued by drug stockouts and aging bed nets that have exceeded their three-year lifespan .
The 2024 El Niño rains served as a reminder of how quickly these systemic gaps can be exposed, causing spikes in transmission among children in poverty-stricken areas with poor drainage . While vaccines offer a high public health impact, their success is tied to the strength of the underlying health system. Without consistent investment in routine care and the replacement of old infrastructure, the protection offered by these new tools risks waning just as the parasite’s resistance rises .
The war against malaria is shifting because the carrier itself is evolving. Groundbreaking research by KEMRI and the Wellcome Sanger Institute has revealed that Anopheles funestus, one of Africa’s most prolific vectors, is far more genetically interconnected across equatorial Africa than previously understood . This genetic “highway” means that resistance mutations present as early as the 1960s are intensifying and spreading across borders with ease, allowing the species to outpace traditional mosquito control tools .
Simultaneously, Kenya is facing an invasion by Anopheles stephensi, an invasive urban vector detected in nine African countries. Unlike native mosquitoes, this invader thrives in man-made containers in cities like Nairobi, bringing malaria into informal settlements already struggling with an escalating crisis of drug resistance . This development creates a new frontline where the disease can strike year-round, unconstrained by traditional rural transmission seasons .
Looking back at the most recent Global Antimicrobial Awareness Week, held between November 18 and 24, 2025, KEMRI researchers provided a grim reality check for urban health centers. Surveillance data from Nairobi’s Mama Lucy Kibaki Hospital revealed that more than 45 percent of typhoid fever cases are now linked to multidrug-resistant Salmonella Typhi, while a staggering 99 percent of Vibrio cholerae strains from recent outbreaks showed similar resistance patterns . This creates a “double front” clinical nightmare: in densely populated informal settlements, healthcare providers are now forced to navigate a diagnostic maze where a patient presenting with a fever could be suffering from a malaria parasite that clears slowly due to genetic mutations, or a bacterial infection that has acquired “drug-defying” genes capable of defeating even our last-line antibiotics . As we prepare for the 2026 awareness week later this year, the priority is no longer just controlling a single disease, but building a multi-pathogen stewardship program that can protect vulnerable populations from this emerging convergence of biological threats .
References:
KEMRI KEMRI Scientists In Landmark Genetic Adaptations of Malaria Transmitting Mosquito Study
KEMRI KEMRI’s Warns of Escalating AMR Crisis in the Country
While Kenya has celebrated a drop in national malaria prevalence from 8% to 6%, a silent mutiny is occurring at the genetic level. Investigative surveillance in eight Western Kenyan counties has confirmed the emergence of k13 gene mutations—specifically A675V, C469Y, and R561H—which confer partial resistance by delaying how fast the parasite is cleared from the blood. Siaya County currently stands as a unique hotspot, harboring all three validated mutations simultaneously, a signal that the parasite is successfully adapting to our primary defense: Artemisinin-based Combination Therapy (ACT).
Research shows evidence of drug-resistant malaria | CGTN Africa
The prevalence of these mutations is shifting regionally, with the A675V mutation rising from 1% in 2022 to approximately 5% in 2023. This specific mutation is predominant in Uganda, suggesting a trans-border biological migration that mirrors the movement of communities across the Lake Victoria region. History warns us that the collapse of a first-line drug, much like chloroquine in the late 20th century, typically leads to a catastrophic spike in mortality across the continent.
Experts describe this as an “evolutionary certainty,” meaning that even our most effective tools will eventually face failure. To counter this, scientists are racing to authorize next-generation, non-artemisinin therapies like ganaplacide-lumefantrine, which achieved positive Phase 3 results in late 2025. For now, the focus remains on scaling up molecular surveillance to catch these “drug-defying” genes before they spread to the rest of the country.
References:
The Scientist The Malaria Fight Evolves: How to Outsmart the World’s Deadliest Parasite
KEMRI | Wellcome Trust Rising K13 validated artemisinin resistance mutations in Western Kenya
Kenya’s public health system is once again on the operating table — but this time, the diagnosis points beyond fiscal failure to institutional betrayal. The government’s May 2024 payout of KSh 3.5 billion in doctors’ arrears briefly restored faith in the state’s willingness to honor past commitments under the 2017–2024 CBA. Yet, beneath the celebration, cracks widened. Barely weeks later, the same administration plunged the sector into chaos over the medical interns’ stipend standoff, slashing agreed pay from KSh 206,400 to 70,000 under the guise of “limited fiscal space.” The ensuing paralysis—interns idled, courts flooded with petitions, hospitals short-staffed—signaled not financial constraint but a governance culture that governs by deferral, treating legality and professionalism as expendable luxuries. What should have been a steady reform agenda has degenerated into episodic crisis management, where every partial solution simply queues up the next emergency.
The deterioration has now metastasized to the counties, where devolved power has mutated into deflection and denial. In Kiambu County, doctors have been on strike for months, accusing the governor of presiding over a “battle of egos” instead of a rescue plan. (The Standard) The Kenya Medical Practitioners, Pharmacists and Dentists Union (KMPDU) has condemned county governments for “derailing progress” by ignoring CBAs, delaying salaries, and politicizing healthcare delivery. The union’s outrage spiked after reports that 131 newborns died amid the Kiambu crisis, a tragedy the Council of Governors publicly dismissed as “false publication.” (Citizen Digital) The KMPDU now demands accountability, an apology, and an independent investigation—warning of a nationwide strike on October 25 if county impunity persists. What began as a county dispute has evolved into a national indictment of how devolution, once hailed as reform, has devolved into an administrative minefield where human life becomes collateral to political vanity.
This crisis extends far beyond Kiambu — it is metastasizing across the entire devolved health network, revealing a structural rot that no press release can conceal. Health workers in Nairobi, Isiolo, Marsabit, and other counties are already on edge over delayed salaries, missing allowances, and ignored CBAs, while local leaders deflect responsibility with ritual blame games. Each county now operates like a fiefdom, where governors weaponize fiscal autonomy to evade national accountability. The result is a patchwork of suffering: hospitals running without drugs, maternity wards closing for lack of staff, and patients dying quietly as politicians trade televised barbs. In this grotesque inversion of priorities, doctors and nurses must fight court battles simply to be paid, while the state spends millions staging health summits and PR drives about universal care. The moral decay runs deeper than bureaucratic failure — it is ethical bankruptcy. Devolution was meant to bring services closer to the people; instead, it has brought corruption closer to the patient. The Council of Governors, once the face of localized empowerment, now functions as a shield for negligence, dismissing human tragedies as “falsehoods” even when families bury their dead. A government that forces doctors back to work through court orders, instead of dialogue, has abdicated the very essence of governance. Every delayed salary and every stillborn infant is a symptom of a political elite desensitized to suffering — one that governs not through service, but through spectacle. Unless the state reclaims discipline, compassion, and coherence in health governance, Kenya’s pursuit of universal healthcare will remain a hollow slogan floating over a silent emergency ward.
References:
The Standard Battle of egos: Counties accused of derailing progress in health sector
Citizen Digital KMPDU slams Governors over Kiambu health crisis, issues demands amid looming national strike
The Standard Doctors to join their striking Kiambu colleagues starting Wednesday
Finn Partners The Evolution of Healthcare in Kenya Amidst Doctor’s Strike and the Rise of Digital Health Innovations
TV47 Kenya Trust deficit is Kenya Kwanza’s greatest undoing” – MP Makali Mulu
Kenya’s 2025 pesticide ban is more than a policy shift—it’s an overdue confrontation with dangerous agrochemical practices that have long gone unchecked. At the heart of the crackdown is Mancozeb, a fungicide so entrenched in Kenyan agriculture that it’s sprayed like water on tomatoes, potatoes, and maize. Yet this widely used chemical breaks down into ethylene thiourea (ETU)—a probable human carcinogen linked to thyroid harm and reproductive toxicity. Mancozeb has already been banned across the European Union and flagged by multiple global health authorities, but until now, it continued to flow into Kenyan markets with barely a check. Now, alongside Mancozeb, Kenya has also moved to restrict or suspend other hazardous products including chlorpyrifos, acephate, glyphosate, and dimethoate—compounds associated with cancer risks, neurotoxicity, endocrine disruption, and acute poisoning in both humans and animals. In withdrawing 77 toxic products and tightening rules on 202 more, the government is finally rejecting the toxic trade imbalance that treats African countries as chemical dumping grounds. The new policy aligns Kenyan regulation with international best practice: no pesticide can be registered here unless it’s also legal in its country of origin and in developed economies like the EU, USA, Canada, or Australia. It’s a turning point—but not without blowback.
A Report by K24TV
For years, Mancozeb symbolized Kenya’s regulatory inertia: cheap, accessible, and unchallenged despite the mounting science against it. Farmers, often unaware of its dangers, sprayed it without masks or gloves, storing the residues in their homes, their soil, and their food. Chlorpyrifos, a widely used insecticide linked to developmental harm in children, and glyphosate, a herbicide under global scrutiny for carcinogenicity, have followed similar trajectories—popular with farmers but flagged by scientists and health agencies. Now, the state faces a high-stakes transition. Smallholders reliant on these chemicals are being urged toward Integrated Pest Management (IPM) and agroecological alternatives. Yet less than 10% of Kenyan farmers use biopesticides, and most lack training, equipment, or trust in new inputs. The Pest Control Products Board, emboldened by fresh legislation, is finally flexing its oversight powers. But enforcement remains patchy, and counterfeit products exploit the regulatory vacuum. Mancozeb isn’t just a pesticide—it’s a case study in how economic expediency once overrode health and environmental responsibility. That era, Kenya now claims, is ending.
Timing is crucial. The EU is cracking down on residue limits. Kenya’s vegetable exports—once worth KSh 100 billion—have already taken a hit. If the country wants to stay competitive and credible, aligning with global safety standards is not optional. Mancozeb’s fall is both symbolic and strategic: it’s a warning to other harmful substances still in circulation—like profenofos, carbendazim, and triazophos—and a test of whether Kenya can enforce its own reform. This is where political will must hold—beyond press briefings and regulatory memos. Farmers need practical support. Consumers need transparency. And regulators must resist the pressure of well-funded pesticide lobbies looking to reverse course. Kenya has declared its direction. Now the country must walk it—with clarity, speed, and resolve—before the next generation pays the price in poisoned soil, sickened bodies, and lost trade.
References:
Trade World News Kenya Bans Import of 50 Pesticide Brands for Safer Farming
The Standard State cracks down on harmful pesticides, bans 77 products
The Star Civil society demand full disclosure of banned pesticides, calls for safer agricultural reforms
The Star 77 pesticides banned in Kenya as 202 others restricted – CS Kagwe
Kenya News Agency State urged to make to make public list of banned pesticides
Kenyans.co.ke Kenya Bans Use of Pesticides Not Approved in Europe, USA, Canada & Australia
When Kenya launched the Social Health Authority (SHA) as the cornerstone of universal health coverage, the promise was clear: to ensure every citizen could access essential health services without facing financial ruin. Yet today, that promise faces a serious credibility test. Recent developments indicate that many Kenyans, particularly the unemployed and low-income earners, are being turned away from public hospitals unless they first settle their full-year SHA premium in advance. This development contradicts the October 2024 assurance that eliminated upfront payments, and it has created uncertainty and distress for millions who had hoped the new system would ease their access to care. While the government’s “Lipa SHA Pole Pole” initiative was introduced as a flexible payment model, its application has exposed a difficult paradox—patients unable to pay full premiums are being directed to loan facilities such as the Hustler Fund, raising concerns about equity and affordability in health access.
A Report by K24TV
The data reinforces the gravity of this policy gap. As of May 2025, around 22 million Kenyans were registered under SHA. However, only 4 to 5 million were actively contributing. This stark difference highlights a growing segment of the population—nearly 17 million—who are nominally enrolled but effectively excluded from coverage. Field reports indicate cases where patients who had made partial payments through monthly KSh 1,030 contributions were still denied treatment unless they completed the full annual sum of KSh 12,460. This shift from previous messaging has created confusion within the public and among healthcare providers alike. Hospitals are left navigating between policy directives and practical enforcement realities, while patients face an impossible choice between debt and delayed care. The concern here is not just administrative inconsistency but a fundamental disconnect between the objectives of health reform and its practical execution.
Efforts to finance the health sector sustainably must not eclipse the foundational goal of protecting all citizens—especially the most vulnerable. Leveraging loan facilities to pay for health premiums, even under a well-meaning “pay slowly” framework, may alleviate cash flow challenges temporarily, but risks increasing personal debt burdens among already struggling households. Basic principles of household economics do not support taking on credit to finance routine health coverage costs—particularly when such expenses are meant to be predictable and pooled through public insurance schemes. Moreover, legal challenges have already resulted in court rulings that bar exclusion from emergency services based on insurance status, underscoring the constitutional imperative of inclusive care. For SHA to regain public confidence, there must be a renewed focus on clarity, consistency, and compassion. Equity must guide implementation just as much as fiscal planning. Universal health coverage cannot be achieved by design alone—it must be delivered through systems that align with the economic realities of those it intends to serve.
References:
The Standard Why most Kenyans cannot access SHA services
Kenyans.co.ke Kenyans Frustrated as SHA Scraps Monthly Payments, Demands Full Year Upfront
GeoPoll Understanding Kenyans’ Perception of the Social Health Authority (SHA) and Social Health Insurance Fund (SHIF)
The Star Jua Kali Kenyans paying Sh600 to SHA—double the promised rate
Kenya’s pharmaceutical supply chain is facing a creeping, deadly crisis — one that’s quietly poisoning public trust in healthcare. In 2024 alone, over 30 different drug products were recalled in Kenya, more than doubling the previous year’s figure. This disturbing surge included contaminated pediatric syrups, mislabeled antibiotics, and packaging mix-ups between life-saving cancer drugs and common generics. Some of these were produced by global manufacturers with once-reputable names. The growing scale and severity of these incidents have exposed glaring weaknesses in regulatory enforcement, border control, and supply chain oversight. But beyond the headlines lies a darker story — fake and substandard medicines are no longer rare exceptions; they are becoming routine features in pharmacies, clinics, and even households. As treatment failures rise and drug resistance intensifies, trust in medicine itself is breaking down. Patients increasingly worry: if I walk into a pharmacy, how can I know what I’m buying won’t kill me?
A K24 Report from 2024
The regulator, the Pharmacy and Poisons Board (PPB), is overwhelmed. With just 16 inspectors tasked with overseeing a vast and evolving market — spanning over 10,000 retail outlets, mobile vendors, and now, an unregulated e-pharmacy explosion — enforcement efforts are falling behind. In 2024, the PPB shut down 117 illegal pharmacies, an important but ultimately symbolic move in the face of thousands more operating without licenses or pharmacist supervision. Online drug sales are the new front line. A study found that over 60% of Kenyan e-pharmacies sell restricted drugs like antibiotics and sedatives without prescriptions, bypassing safeguards entirely. These platforms, often disguised as Instagram shops, WhatsApp-based vendors, or websites with fake credentials, target desperate buyers looking for cheap, fast relief. With little digital verification, no pharmacist involvement, and no legal framework to manage or penalize them, the risk of mass harm is escalating. Meanwhile, legitimate pharmacies face the fallout: eroded consumer confidence, a rise in self-medication, and unfair competition from black-market sellers. At the center of it all is a poorly resourced regulator trapped in a battle it cannot win with its current tools.
Fixing this won’t come from a few more closures or stern warnings. What’s needed is a total overhaul of pharmaceutical regulation and public health literacy. The PPB needs financial and legal independence, an expanded workforce, and modern tools — including barcode authentication, blockchain-backed tracking systems, and real-time reporting dashboards for drug recalls and falsifications. E-pharmacies must be brought under legal oversight immediately, with criminal penalties for non-compliant platforms. Consumer protection should no longer be passive; the government must launch aggressive national awareness campaigns to teach people how to identify fake drugs, report suspicious sources, and verify prescriptions. Crucially, Kenya must repair public trust — not just in the pills on pharmacy shelves, but in the very systems meant to safeguard their health. Because when faith in medicine collapses, people don’t stop getting sick — they just stop getting help. This is more than a regulatory failure. It’s a national health emergency — and one that cannot be ignored.
Faced with a deepening maize crisis and the threat of unaffordable unga prices for millions of households, the Kenyan government has authorized the importation of yellow maize under a 50% duty waiver. The policy aims to ease the strain on white maize—Kenya’s staple grain for human consumption—by diverting demand from feed manufacturers. By encouraging millers in the animal feed industry to substitute white maize with yellow maize, the government hopes to reduce competition for white maize, making it more accessible and affordable to food processors and, ultimately, to consumers. However, this economic intervention carries unintended consequences that could undermine its goals. Due to Kenya’s fragmented supply chains and patchy enforcement mechanisms, experts warn that the clear division between maize meant for animals and that meant for humans may not hold. The significantly lower price of the imported yellow maize could tempt unscrupulous traders to redirect it into the human food market—either by blending it with white maize flour or selling it directly in low-income areas where yellow maize is already accepted as food, such as parts of Western Kenya. In places like Homa Bay County, where yellow maize is widely consumed in the form of ugali, this policy shift could unintentionally flood the food supply with grain that may not meet safety standards for human consumption.
A Report by NTV Kenya
The core of the concern lies in the persistent and well-documented threat of aflatoxin contamination, a toxic compound produced by mold that thrives in warm, humid conditions—particularly in improperly stored grains. While Kenya has established aflatoxin limits aligned with East African Community standards—10 parts per billion (ppb) for total aflatoxins and 5 ppb for aflatoxin B1—systemic challenges hinder enforcement. Many small-scale producers, informal traders, and millers lack access to the sophisticated equipment and financial resources needed to test for aflatoxins or implement preventive storage solutions. Furthermore, there have been troubling precedents that cast doubt on the robustness of regulatory oversight. In 2011, a shipment of aflatoxin-contaminated maize from the U.S. was allegedly released into the market despite being flagged by authorities, with reports suggesting that the Kenya Bureau of Standards (KEBS) was blocked from conducting proper inspections. More recently, in January 2025, a 2,000-tonne shipment of rice from Pakistan was found to exceed aflatoxin limits, indicating that lapses in import control remain a pressing issue. These incidents demonstrate that having regulations on paper is not enough—especially when imports labeled for animal feed, which undergo less rigorous scrutiny, may be co-opted into the human food chain in the absence of strict monitoring, reliable segregation mechanisms, and transparent accountability.
The potential health implications of increased aflatoxin exposure are grave and far-reaching, especially for vulnerable populations who rely heavily on maize as their primary food source. Acute exposure can lead to severe liver damage, jaundice, and even death, while long-term, low-level exposure is linked to liver cancer, immune system suppression, nutrient malabsorption, and developmental issues in children. Infants and young children face elevated risks due to their small body mass and the fact that complementary weaning foods are often maize-based, yet specific aflatoxin regulations for these products are either absent or poorly enforced. For populations with pre-existing liver conditions, Hepatitis B infections, or compromised immunity—such as people living with HIV—the health risks are significantly amplified. Malnourished individuals and rural subsistence farmers, who often rely on their own poorly stored harvests, are also at heightened risk. In the face of this looming danger, health advocates and food safety experts are calling on the Kenyan government to urgently invest in comprehensive and well-coordinated countermeasures. These include rigorous aflatoxin testing of all maize imports, stricter enforcement to prevent feed-grade yellow maize from entering the human food stream, large-scale public education campaigns targeting high-risk regions, and long-term investments in improved post-harvest storage infrastructure. Without such measures, the policy designed to stabilize food prices could inadvertently trigger a public health emergency—one that disproportionately affects the country’s poorest and most vulnerable.
References:
Nation Kagwe bows to pressure, opens imports as unga prices hit 13-month high
Jijuze Maize Prices Surge: Impact on Kenya’s Livestock and Food Security
Kenya’s mental health sector presents a striking paradox: despite the growing recognition of mental health challenges and an increasing demand for psychological services, psychology graduates continue to face significant unemployment and underemployment. This contradiction is rooted in deep-seated structural issues that systematically undermine the profession, making it difficult for trained psychologists to secure stable, well-paying jobs. One of the primary factors contributing to this crisis is the severe lack of job opportunities within both the public and private sectors. Many organizations, including hospitals, rehabilitation centers, and educational institutions, employ only a minimal number of psychologists, often restricting these roles to one or two individuals per institution. This results in a highly competitive job market where only the most experienced professionals stand a chance of securing employment, leaving recent graduates with limited options. Additionally, the financial sustainability of private practice is severely threatened by the prevalence of free or low-cost counseling services offered by religious institutions, non-governmental organizations, and community-based groups. While these services play a crucial role in expanding access to mental healthcare, they inadvertently undermine the ability of qualified psychologists to establish viable independent practices. Consequently, many graduates are unable to leverage their expertise in the field, often resorting to working in unrelated sectors, taking on temporary and poorly remunerated jobs, or abandoning the profession altogether despite their years of specialized training.
A Citizen Digital Report on Mental Health Awareness
A major challenge compounding this issue is the lack of a structured and regulated career pathway for psychology graduates, which creates uncertainty for both practitioners and potential employers. Unlike other fields such as medicine, law, or engineering, where licensing and professional development are clearly defined, psychology remains a largely unstructured profession in Kenya. The absence of standardized guidelines for internships, supervised practice, and professional accreditation means that many graduates complete their studies without the practical experience necessary to meet employer expectations. This situation is further exacerbated by the commercialization of mental health services, where some institutions prioritize financial gain over the provision of quality care. This business-oriented approach has led to exploitative employment conditions, where psychologists are often hired on short-term contracts with little job security, minimal benefits, and unrealistic workloads. Furthermore, some rehabilitation centers and private institutions reportedly prefer hiring new graduates on temporary terms rather than renewing contracts with existing employees, ostensibly as a cost-cutting measure to avoid higher salary commitments. These systemic challenges not only create instability within the profession but also discourage qualified individuals from remaining in the field, ultimately reducing the availability of experienced professionals in the country’s mental health workforce. As a result, Kenya continues to experience a significant gap between the increasing need for psychological services and the limited number of trained professionals who can afford to remain in practice under these conditions.
Addressing these issues requires comprehensive structural reforms aimed at professionalizing the psychology field and integrating it more effectively into Kenya’s healthcare and social support systems. First, policymakers must acknowledge the critical role of psychology in national development and mental well-being by increasing investment in mental health services, expanding employment opportunities within public institutions, and ensuring that psychologists are recognized as essential healthcare providers. Universities should also play a more active role in bridging the gap between academic training and practical application by incorporating robust internship programs, mentorship opportunities, and entrepreneurial training to equip graduates with the necessary skills to navigate the job market. Additionally, regulatory bodies should establish a standardized licensing framework to ensure that all psychology professionals meet clear competency standards while also receiving fair remuneration and workplace protections. By implementing these reforms, Kenya can begin to address the persistent challenges facing psychology graduates, ensuring that their skills and expertise are fully utilized to meet the country’s growing mental health needs. Failure to take action will not only continue to render psychology graduates underemployed but will also undermine the long-term development of the mental health sector, leaving thousands of Kenyans without access to qualified psychological care at a time when it is needed more than ever.
References:
Nation Psychology graduates struggle to get jobs in Kenya
Nation THE SILENT SCREAM OF KENYA’S PSYCHOLOGY GRADUATES
The Star Tales of despair for Kenyan graduates seeking jobs
Johnson & Johnson Building health worker capacity to close the mental healthcare gap across Kenya